Daily News 11 June 2018 a Self-balancing Exoskeleton Lets Wheelchair Users Walk Again
1. Introduction
Walking that is significantly dissimilar from a normal gait is called an abnormal gait. Abnormality of walking can be generated by various causes, such as muscular weakness, paralysis, pain, limited range of motion, neurological disorders, and leg length discrepancy. Diseases that tin cause abnormal gait include stroke, cognitive palsy, and Parkinson'due south disease. For example, afterwards a stroke, most patients experience weakness or paralysis on i side of the body, and many of them too experience spasticity [i]. Due to the weakness of distal muscles, hemiplegic patients drag their legs in a semicircle. Additionally, patients with Parkinson's disease have a shuffling gait due to basal ganglia dysfunction. They may experience freezing at the beginning of their walk or may have a festinating gait during walking. Another representative cause of abnormal gait is cognitive palsy. Abnormal gait due to cerebral palsy includes equinus gait, crouch gait, jump human knee, and drop human foot or a simultaneous combination of these symptoms.
Therefore, abnormal walking occurs in the event of an abnormality in the sensory and motor systems that activate certain muscles. If the Hamstring weakens, a hyperextension of knee joint occurs in the stance phase and the human knee is not flexed in the terminal swing and continues to extend. Furthermore, if at that place is an abnormality in hip abductor muscles, gluteus medius gait occurs, in which the torso leans over the opposite leg during the swing phase. Articulation pain and weakness due to aging also crusade abnormal walking. Frank et al. showed that muscular strength declines with historic period and decreases past up to 50% by the age seventy [two]. Patients with aberrant walking and rest disorders are afraid of walking and cannot walk for a long time. These mobility disabilities increment the risk of dependency in physical activities in daily living [2,3].
If abnormality is not considerable, balancing can be assisted by a simple walking aid such equally canes, walkers, crutches, then on. Using these, the base of support can exist widened to help maintain balance [iv]. Withal, when used for a long time, the arm muscles may get painful. In some cases, an Ankle Pes Orthosis (AFO) or a Genu Talocrural joint Human foot Orthosis (KAFO) is used to companstate weakness. There are various materials and structures of orthosis; recently, electrical devices that incorporate active joints have been introduced [v].
For people with partial impairment in walking ability, information technology is mandatory to stand up and perform walking motions frequently with the help of assistive devices (eastward.g., a harness organization, a robotic rehabilitation treatment organization, etc. [6]) to maintain health conditions. In this respect, clothing robots enabling the patients with paretic gait walk on the real basis tin can exist used. These robots are constructive both for rehabilitation and for an increase in the patients' mobility.
In recent years, clothing robots for gait aid accept been developed and commercialized [7]. Among many applications of the wearable robots, ones for assisting people with complete paraplegia may exist the mostly popularized. While wheelchairs tin can better the mobility of patients with consummate paralyses, they cannot provide standing postures and bipedal walking, which are important for healthcare. Many studies have shown that bipedal walking training tin increase quality of life and life satisfaction [half-dozen,8,ix,10]. ReWalk, a commercial robot by ReWalk Robotics [11], is currently being distributed to rehabilitation hospitals effectually the world. Other commercially available robots for disabled and paralyzed people are Ekso [12] from Ekso Bionics, Indego [xiii] from Parker Hannifin corporation, and Rex [14] from Rex Bionics. Many other robotic exoskeletons are being adult and commercialized [15,xvi].
In such cases of a vesture robot for complete paraplegics, i.e., people with complete loss of walking power, it is mutual to use a position tracking control scheme. There are cases where position tracking control is used in robots for people with fractional harm in walking ability, such as hemiplegic or stroke patients [17]. This allows the user to imitate the trajectory of a normal gait or the trajectory of a healthy side leg. However, for incomplete paraplegics with remaining sensory and motor functions, the position command strategy constrains the human'southward voluntary motility, and thus, the wearers of such robots take to learn to suppress voluntary move and to fully rely on the robot. This may non be appropriate in the viewpoint of rehabilitation medicine, and at present, it is hard to observe a habiliment robot that tin compensate but for the lack of the weakness of muscular power without disturbing a human's voluntary motions. In that location are soft article of clothing suits, but such soft a machinery is non suitable to help cocky-balancing of people with muscular weakness [6,xviii].
For gait rehabilitation and assistance of people with partial harm of walking power, a torque control method may exist more constructive. The torque control is a method that allows the user to control the movement while allowing the advisable aid at the required moment, such equally pushing the swing from backside. Therefore, there is a clear need for a control method that captures the exact moment when assistance is needed and provides equally much assistive torque every bit needed.
The master aim of this paper is to improve the walking of patients with paretic gait by applying the torque assist algorithm using a habiliment robot. In order to attain this goal, the following objectives are formulated:
-
integration of torque-way actuators and a wearable robot,
-
development of a real-fourth dimension gait detection algorithm with simplified gait phases,
-
generating a patient-customized assistive torque and control algorithm, and
-
validation of the consequence of walking assistance using the proposed wearable robot through a case study.
ii. Angel Legs: A Powered Exoskeleton with Torque-Mode Actuators
Parts of this section accept been previously presented in [19].
In this paper, Angel Legs, the powered exoskeleton shown in Figure 1, is introduced. The proposed robot has been especially designed for assisting people with partially impaired walking ability. In recent years, assistive robots for people with partially dumb walking ability are being commercialized by a few research groups. Cyberdyne Inc., Tsukuba, Japan, a popular wearable robot company in Japan, has developed the HAL series. ReWalk has launched a soft exo suit, called ReStore, for assisting stroke patients [20]. The existing products, however, may non still provide a practical and bonny solution to real-world users considering they require attachment of electric sensors on the nude skin and impose a big resistance on the human joints due to actuator friction. Robotic aid with a large actuator friction may not be the correct solution for people with partially impaired walking ability. The soft exo suit is very promising in this aspect, merely information technology is non suitable to help maintain the whole-body rest of a patient due to the characteristics of the soft mechanism. Considering these aspects, Angel Legs has been adult based on series elastic actuation (Body of water) systems, which enables accurate assistance with almost-zero mechanical impedance [21], i.e., "transparent assistance".
The design of Affections Legs demands unique requirements, such equally minimal mechanical impedance and high back-drivability, too as high power density. The mechanical parts must exist ergonomically designed, such that humans tin can use the devices for a long menses of fourth dimension without discomfort. The motor control function of people with impaired walking ability is non every bit robust as that of the normal, and thus, the overall human body system becomes vulnerable to disturbances (i.e., external forces, inclinations, etc.) or model variations (i.due east., loads, etc.). It is, however, still agile, unlike consummate paraplegic patients, and thus, the robot must not generate whatsoever unexpected resistance confronting the voluntary motions of people with impaired walking ability for condom and for minimal discomfort. Therefore, both the design and control of assistive robots for people with partially impaired walking ability are very challenging. As the muscular strength of the target users is weakened (but not fully impaired), the overall weight, the actuation resistance and precision, and the condolement of the robot hardware have ever been the main concerns in the mechanical blueprint of Angel Legs.
two.1. Ability-Pack System
Angel Legs includes a high capacity battery pack made of lithium-ion cells. The nominal voltage of the battery pack is 44 V, and the free energy capacity is 3 Ah, which is skillful for profitable walking for nigh two hours. To provide a big electric electric current to the electric motors, in item, to initiate motion at a stall state, battery cells with a loftier C-charge per unit are utilized. The nominal voltage is selected at 44 V considering the relevant international standard (e.g., ISO13482) states that a voltage under 50 V is regarded as safe.
The bombardment pack can be replaced hands. When the battery pack is fully discharged but the user wants to continue activities without recharging the battery, it tin can be disassembled past only opening two latches placed on both sides of the battery pack and tin be replaced with a spare battery pack. The bombardment pack is controlled by a loftier-performance battery management system (BMS). The functions of the BMS include (one) over-charge and over-belch protection, (two) over-electric current protection, (3) electric short protection, (4) battery cell temperature monitoring and control, then on. In add-on, the BMS balances the remaining energy in each of the battery cells, such that all the bombardment cells tin can be equally charged and discharged. The BMS frequently reports the condition of the battery pack to the main processor (i.e., NI sbRIO-9651) via the I2C communication. The remaining battery energy is displayed at the primary control console.
ii.2. Actuation Organization of Angel Legs
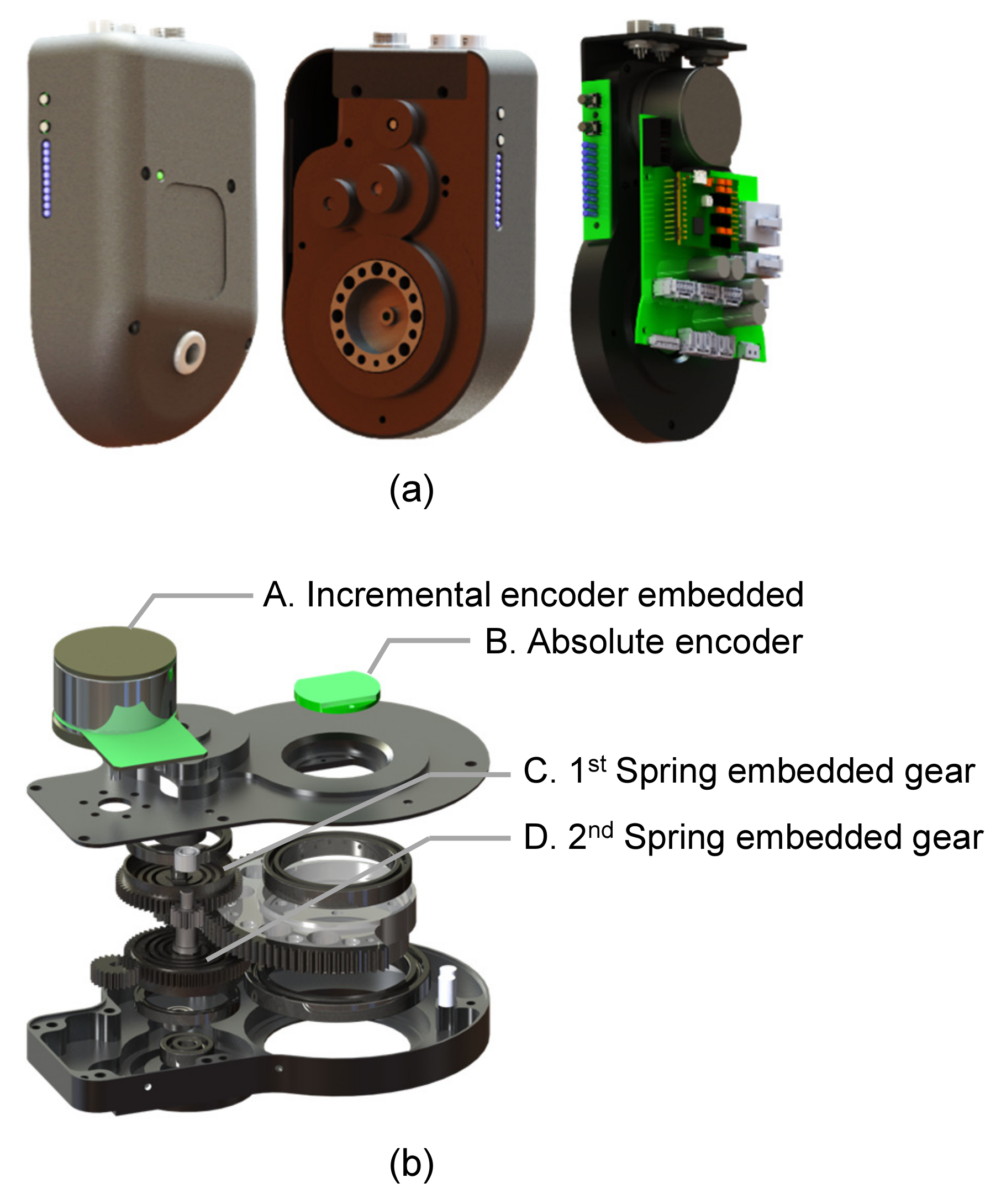
An actuation module of Angel Legs, called Angel Joint v1, is shown in Figure 2. For accurate control of the assistive torque transferred to the human joint, a structural spring is utilized, as shown in Figure 2b, which realizes the serial elastic actuation. The spring plays the roles of an energy buffer and a torque sensor [22,23]. By measuring the spring deflection, the assistive torque tin can be measured. Therefore, the precise torque command can be achieved past decision-making the spring deflection. In addition, the spring is helpful in improving the safety of the actuation module.
Angel Joint v1 consists of a castor-less direct-current (BLDC) motor (Maxon motor company, seventy W, EC45-flat), jump-embedded gears, sensors for measuring the spring deflection, as well as the absolute angle of the human articulation. However, the actuation power is not very meaningful because the motor is operated at low speeds, where the stall country takes a place often. After the gears and a spring, the magnitude of an assistive torque is about
Nm in a continuous assist condition and
Nm in a short-term assist condition. The other mechanical specifications are shown in Tabular array ane.
The actuation performance of Affections Joint v1 is determined by the design of the spring-embedded gears as well as a control algorithm decision-making the bound deflection. As shown in Figure 2b, Angel Articulation v1 is designed to have two spring-embedded gears. For the sake of minimal weight and volume, the "spring-embedded" gears embed springs, such that the gears showroom elasticity without any additional springs. Every bit the spring-embedded gears should be made of a strong material to forbid the failure of gear teeth, the jump constant is unavoidably high. Therefore, Angeloint v1 has ii leap-embedded gears to realize the desired bound constant.
Figure 3 shows the linearity of springs in the Angel Joint. It was measured by a dynamometer. The leap constant was measured past
Nm/rad and the backlash, i.east., the dead-zone at the zero-torque shown in Figure 3 was measured as
degrees (i.e.,
rad. The backlash was acquired by the tolerance of gear teeth, and the torque measurement error due to the backlash was about
Nm, i.e.,
Nm/rad ×
rad. This error is small-scale plenty compared with the magnitude of desired assistive torque (i.east.,
Nm).
2.three. Torque Control Algorithm
I of the most unique characteristics of Angel Legs is the "transparent" actuation, i.e., precise torque control without resistance. The transparent actuation is realized past the command of the jump deflection in a series elastic actuator. Effigy 4 shows the command block diagram of the transparent actuation. The desired (i.e., reference) assistive torque (
) is loaded when the user selects the operation mode through user interface systems, such as a tablet device and an embedded controller push button. Past Hooke's law,
is and then converted into the desired angular position of the motor (
), i.e.,
, where
and one thousand are the human being joint angle and the spring constant, respectively.
The encoder signals (i.east., a pair of an absolute encoder and an incremental encoder for each actuation module (see A and B in Figure 2b)) are utilized for measuring
and
. Equally the human being articulation angle may include a measurement error due to the inherent characteristic of a magnetic encoder,
is compensated by a pre-obtained compensation indicate (see (a) in Figure 4).
The motor athwart position can be accurately controlled to follow
based on the position command method. In Angel Joint v1, a proportional-integral-derivative(PID) controller (come across (b) in Figure iv) and an impedance compensator (see (d) in Figure iv) are implemented for position command. The PID controller gains are inverse co-ordinate to the magnitude of the torque fault (see (c) in Figure 4).
Once the motor is accurately controlled, the spring deflection is accurately controlled, which implies the authentic command of assistive torque.
3. Real-Fourth dimension Gait Detection Method
3.one. Classification of Gait Phases
Homo walking can be regarded as a periodic movement composed of several phases. Using insole sensors with two sensors on a foot (i.e., toes area and heel area), four phases can be detected; heel strike, mid stance, terminal stance, and swing. However, if the leg muscles or joints are weakened or damaged, the sub-phases of the stance phase (i.e., heel strike, mid opinion, and terminal opinion) may not be obvious in gait analysis. For case, patients with equinus gait (i.east., tiptoe gait) do not impact their heel to the ground during walking. In this example, a gait tin can be classified into two master stages: (one) a stance phase in which whatsoever part of the foot touches the ground and (two) a swing phase in which the pes is completely off the ground. Figure 5 shows the simplified gait phases of a leg. Because the phase of the opposite leg, the opinion stage of the leg can be divided into the first double limb support phase (DS1), single limb support phase, and the second double limb back up stage (DS2). Therefore, the gait can be classified into four index phases every bit follows.
-
Gait index 1: Double limb back up with the correct leg forwarded (DS1)
-
Gait index 2: Unmarried limb support of the right leg (left swing)
-
Gait index iii: Double limb back up with the left leg forwarded (DS2)
-
Gait index iv: Unmarried limb support of the left leg (right swing)
The double limb support stage of the right leg includes the stance stage of the left leg, and the unmarried leg support phase of the right leg means the swing phase of the left leg. Therefore, the proposed four-level classification covers the entire gait phase of both legs. People with paretic gait mostly have longer double limb back up times than healthy people. Except for those who are severely paralyzed or lack muscle strength enough to exist unable to lift their legs at all, people walk in sequential phases when walking forward.
3.2. Gait Detection Algorithm
In this section, the gait index derivation from the measurement of the foot sensor-pad during walking is introduced. In the example of people with paralytic gait, the swing motion is performed only when the heart of gravity is stable. Therefore, the timing of the initial swing depends on the intention of the person. Robotic support for incomplete paraplegics should likewise be practical when the person intended. Otherwise, the operating strength will cause unstable movement of humans and robotic systems. In this newspaper, the walking intention is monitored in real-time through the gait index analysis method using the foot sensor pad.
Swing phase of a leg tin can exist determined equally
:
where
and
are the measurements of the toe and heel sensor pads, respectively, and southward is the threshold to check that the sensor is pressed. Figure 6a shows the swing phases of both leg while walking, and
represents the stance phase. As described in Section three.ane, the gait can be classified into four phases. To switch the control scheme according to the gait phase, it is necessary to observe the moment of phase change.
The falling border of
represents the initial contact event of the right leg, which is equivalent to
, the rising border of
is equivalent to
, the falling edge of
is equivalent to
, and the rising edge of
is equivalent to
. The derived gait alphabetize of walking is shown in Figure 6b.
four. Articulation Torque Assistance Control
4.1. Assistive Command
As the actuation modules can generate assistive torques accurately, Angel Legs is able to assist the human motion following the "assistance as needed" strategy [24]. Effigy 7 shows the overall aid control method of Angel Legs. The gait intention detection algorithm makes a triggering signal according to the ground reaction force(GRF) signals and the hip and knee joint angles. Then, the desired assistive torque is generated co-ordinate to either (i) a wait-up tabular array or (2) a feedback algorithm, which should be selected depending on the help strategy for each individual user. The desired assistive torque is transferred to the torque command algorithm in Effigy vii and and then the user is assisted with the actual assistive joint torque.
The assistance parameters should be adjusted for each individual user. Angel Legs can provide more natural help if adjusted for each user. The personalized assistance modes, the level of assistance, the range of movement of joints, etc. tin be adjusted. The case shown in the Figure 8 is the predefined torque profile (i.e., the expect-up table method). Through the tablet computer, the user can adjust the instances and magnitudes of peak torques, and so, the remaining parts are automatically interpolated to prevent any discontinuous or impulsive torque.
four.2. Design of an Assistive Joint-Torque Profile
Although human being motion is not generated past a rotary actuation on a single centrality joint, the sagittal joint torques (i.due east., articulation moments) can exist estimated by using inverse dynamics. During stance phases, both hip and knee joints need extension torques to resist and propulsion, and flexion torques required to button forward the swing side leg. People with incomplete paraplegia take a lack of muscle strength, making information technology difficult to push the forelimbs forward, and have a short swing period. Therefore, in one case the initial swing is detected, the assistive torque should be provided for an appropriate amount of time and so that the wearer can use the assistive torque through repeated practise.
For private gait training, it is necessary to hands modify the assistive torque profile without compromising the continuity of the trajectory function. Therefore, polynomial functions were used in this research to find the equations for joint torque trajectories. In addition to the weather condition mentioned above, the derivatives at the beginning and end of the gait should be null in order to smoothly switch to other motions such every bit standing. No other inflection points should exist between the main points. Therefore, we divided the trajectory to four sections based on the main points, and the 3rd order polynomials were derived for each section.
While
means the representative point of the torque trajectory, where
is the percentage of gait cycle and
is the reference torque, the coefficients of polynomials can be derived equally below.
the inverse of which is
Therefore, the articulation torque profile of hip articulation can be expressed as
Figure 8 shows the assistive torque profile based on the gait phases. The representative points
and
, i.due east., the maximum points of flexion and extension torques of hip and knee joints, tin be individually set. The assistance instance is based on the users' gait phases. For the right leg, (a) in Figure 8 is the same every bit
(i.eastward., right contact), and (b) is the aforementioned as
(i.e., left toe-off). In this case, the time between (a) and (b) can not be predetermined since it truly depends on the users intent. When the user tries to move the hind leg for a swing movement, then
is detected and the assistive torque corresponding to those between (b) and (c) are applied. Although the fourth dimension of the (c) is non exactly the same every bit the actual
, which as well depends on the user's intent, the same assistive torque of fourth dimension (c) is practical until (d), i.e.,
. Similarly, the torque of (e) (i.e.,
) continues until the side by side gait event
.
The amplitudes of the peak torque tin exist adapted depends on the patient'southward muscular strengths of each leg and desired aid level. Based on the moments on normal gait with healthy people [25,26], the superlative moments for normal walking can exist assumed as
and
Nm/kg for
and
, respectively, and
,
, and
Nm/kg for
,
, and
, respectively.
5. Verification of Rehabilitation Effectiveness with a Case Report
This department introduces a case study with Angel Legs. The participant in this paper was an 11-year-old female with incomplete paraplegia caused by spina bifida. In full general, the musculus strengths of her lower extremities were form 1/v to 3/5 on the Medical Enquiry Quango calibration. Figure 9 shows the scene of the motion capture-based gait assay. The human being subject was able to walk on the flooring wearing solid talocrural joint-foot orthoses. She had a large deviation in left and right musculoskeletal functions and had to apply trunk muscles to move her pelvis and legs. She also could not walk for a long time, then she used a wheelchair near of the fourth dimension. Due to excessive pelvic inductive tilting caused past hip extensor weakness, the hip joints by and large bent forward and showed fiddling extension. During walking, the left and right hip joints could not be sufficiently stretched to the back and were aptitude by more than than twenty degrees, which caused back pain when walking for a long time. Due to differences in left and correct muscular strengths, at that place was a pregnant difference betwixt the left and right sides in the stance periods and the range of motions of the genu. Since the correct side muscle was weaker than the left side, the right stance menstruum was shorter than the left opinion period.
Parallel bars are the well-nigh commonly used method in the early stages of gait training for rehabilitation. This method helps patients become more confident most using walking equipment, such equally crutches, canes, and walkers. In what follows, we describe the results of several assistive methods using Angel Legs, a torque-controlled wearable robot. Walking with parallel bars, wheeled walkers, and bilateral forearm crutches were attempted and and then analyzed (Figure 10).
5.one. Assistance with Parallel Bars
In the case of torque-based control, we applied the walking intention detection algorithm using insole pad sensors. The gait index was detected by the algorithm in real-time, and the robot provided the assist torque corresponding to the gait alphabetize.
Figure 11 shows the kinematic results of the gait training with and without torque assistance of the robot on the parallel confined. In the case of walking using parallel bars, the typical photographic camera-based motion capture system could not be used, since the body markers were blocked past parallel confined. Therefore, the gait information was acquired using the sensor system. Due to torque-based assistance, the difference in the left and right stance phases was reduced.
Equation (v) was used to make up one's mind the gait symmetry. Symmetry Index (
) was defined as follows:
where
is the value of the non-injured side, which can exist the left side in this case (i.e., the gait percentage of the stance phase), and
is the value of the correct side [27]. The gait symmetry index in the opinion stage was improved from 15.07% without torque assistance to −two.69% with torque assistance.
5.2. Assistance with a Wheeled Walker
Afterward three weeks of training, the patient started basis walking with the help of a wheeled walker wearing Angel Legs. The intention detection algorithm was applied, and on each trial, she walked over a track of 20 k in length (Figure 12).
Figure xiii and Table 2 testify the kinematic results of the hip and knee joint joints of left and right legs and the gait parameters of a walking trial. The solid lines represent the mean value of the total gait. The gait symmetry index in the stance stage improved from 22.48% without robot aid to 4.08% with torque assistance.
To institute the effectiveness of the torque assistance of the proposed robot, nosotros analyzed the following two cases. The offset case was walking with robot help using a walker, and the second case was a walking without robot aid using a walker. The vi-min walking exam measured energy consumption by measuring walking distance, oxygen consumption, and heart rate.
According to the results of the 6-min walking test, the walking distances were 62.92 m and 61.84 k without and with torque aid of the proposed robot, respectively. In these two weather condition, the average center rates were very like: 123.vii and 123.8, respectively. Table 3 shows the results of the oxygen cost assay: 1.35 mL/kg/thou in the no robot support status and 1.76 mL/kg/one thousand in the robot back up status.
5.three. Help with Forearm Crutches
In this experiment, bilateral forearm crutches that allowed the patient to utilize their left and right artillery more freely than a walker were used. Equally shown in Effigy 14, the patient wore the proposed robot and used bilateral forearm crutches. Using bilateral crutches, she could stand straighter than using a walker. The bilateral crutches facilitated rest motion between the left and right sides. For five weeks, one hour of the robot walking training using bilateral forearm crutches was conducted every week. After five weeks of training, two 6-min walking tests of walking with robot assistance and without robot assist were conducted.
Effigy 15 shows the results of the five-week gait training. The kinematic results were derived from the hateful of 20 m path walking for each grooming. The lightest blueish line indicates the first weeks' data, and the darkest blueish line indicates the fifth weeks' data. The vertical line represents the opinion phase of the gait cycle.
As shown in Figure 16a, the opinion phase period decreased as the grooming was repeated weekly, and this may exist seen equally an increment in walking speed. Figure 16a provides a visual representation of the stance phase menstruum changes and the opposite human foot-off menses changes. As a result of repeated training, the single limb continuing time increased (see Figure 16c).
Tabular array 4 shows the results of the kinematic gait analysis of the motion capture arrangement of robot walking using bilateral crutches. No significant differences betwixt the left and correct values of all the gait parameters were observed. The gait symmetry index in stance phase improved from 13.53% without robot assistance to −1.10% with torque assistance, which was similar to the alphabetize of the walking of healthy people. Figure 17 shows the results of walking without robot assistance and walking with robot assist using bilateral crutches. In the instance of the walking with a torque-controlled robot, the hip joint was fully extended and the range of motion of the articulatio genus joint increased.
Throughout the 10-week robot walking training, the patient became accustomed to the robot walking and found an optimal walking pattern using the assistive force of the robot. As in Figure sixteen, the duration of the stance phase decreased with time, similarly to that of the normal gait, which was as well associated with an increase in single back up time. In add-on, the patient'south existence familiar with walking methods using bilateral crutches and learning the patterns of torque aids reduced her fear of malfunction.
Table 5 shows the oxygen cost results of the 6-min walking test using bilateral crutches. According to the experimental results, after five weeks of training, the energy consumption in the walking with robot assistance was 30% less than in the walking without robot aid.
5.iv. Assistance with Increasing Genu Extension Help
During the case written report, the patient experienced difficulty in weight bearing due to muscle weakness. The extension torque help of the opinion phase and the flexion torque assist of the swing phase were constructive in the curt- and long-term gait trainings. In social club to observe the alter in gait patterns according to the magnitude of the extension torque of 1 side (the weaker side), in item, the 20 m path walking tests were performed using different torque profiles on the same training day.
The walking data for iii different weather condition were nerveless. As shown in Figure eighteen, the extension torque of the stance stage of the correct genu was unlike in each status. In each example, the extension torque level of the right knee was set to
,
, and
% of normal walking.
Effigy 19 shows the kinematic results of the 3 trials shown in Effigy 18. No significant difference in the left and correct stance phase periods was observed; however, with an increase of the right knee extension assistive torque, the hip extension range increased.
The results of the analysis of gait parameters are shown in Table 6. In trial 3 and trial 1, the maximum hip extension angles of the left and right were
and
degrees greater, respectively. The first double support stage on the right can be considered to indicate the weight support preparation for the left swing. With an increment of the extension torque, the difference between the right and left of the double support stage reduced.
half-dozen. Conclusions
In this paper, a method to assist the walking of people with paretic gait using a powered exoskeleton, chosen Angel Legs, was proposed. First, an algorithm that uses a sensor system to determine the user's real-time walking pattern and intention was proposed. The gait parameters were derived from continuous walking data, and the abnormality of walking was confirmed. Based on an understanding of the gait pattern, control algorithms that provide adequate assistance were as well discussed. General equations for assistive torque generation were introduced. These equations can be adjusted for each private based on personal musculoskeletal characteristics.
To verify the proposed organization, a instance study with an eleven-year-former female child with a discrepancy in leg length and aberrant deformities due to congenital spina bifida was conducted. At the early on stage of the preparation, by using the proposed torque aid robot, the walking symmetry index improved from 22.48% to 4.08%. At the end stage of the weekly repetitive gait training, the oxygen cost in the 6-min walking examination decreased by 29%, from 1.93 mL/kg/chiliad to 1.37 mL/kg/m.
Considering that oxygen cost is direct related to gait inability [28], this consequence demonstrates that gait inability in robot walking improved through training. Through the ten-week robot walking training, the patient grew accustomed to the robot walking and institute an optimal walking design using the assisting torque of the robot. As shown in Figure sixteen, the ratio of the stance phase in gait bicycle was almost threescore%, which is similar to that of normal gait. In particular, Figure xv shows genu flexion in the commencement double support period of the right leg, i.due east., in the loading response section. This feature did not appear at the early stage of the training, which shows that the integrated organization of the patient and the robot started to employ the assistance force of the robot in an energy-efficient way. In addition to kinematic and metabolic improvements, the patient's feedback was as well positive. Earlier gait training, she did not sense filling of ber bladder; later on the training, her urinary role and quality of life improved.
In the near future, robotic gait grooming proposed in this newspaper for patients with cognitive palsy who have spastic paralysis volition be applied. Past increasing the number of cases and patients, the effectiveness of long-term preparation with regard to various indicators will exist examined. Assistive methods for various tasks, such equally stair climbing, sitting, and continuing, will also be studied.
Funding
There is no funding agency to report.
Institutional Review Board Argument
The study was conducted co-ordinate to the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Lath of Severance hospital, Yonsei university college of medicine (four-2016-0167, approved on 20 April 2018).
Informed Consent Statement
Informed consent for participation was obtained from the parents of the kid in this newspaper according to the rules of the IRB of Severance hospital.
Acknowledgments
The authors would similar to give thanks C. Park for participation in the example report and B. Na for the pattern and development of the robot hardware.
Conflicts of Interest
The funders had no role in the design of the study; in the drove, analyses, or estimation of data; in the writing of the manuscript; or in the decision to publish the results. There are no conflicts of interest from the authors.
References
- Zorowitz, R.D.; Gillard, P.J.; Brainin, Thou. Poststroke spasticity Sequelae and burden on stroke survivors and caregivers. Neurology 2013, 80, S45–S52. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.Southward.; Patla, A.E. Balance and mobility challenges in older adults: Implications for preserving community mobility. Am. J. Prev. Med. 2003, 25, 157–163. [Google Scholar] [CrossRef]
- Hirvensalo, One thousand.; Rantanen, T.; Heikkinen, E. Mobility difficulties and physical activity equally predictors of mortality and loss of independence in the customs-living older population. J. Am. Geriatr. Soc. 2000, 48, 493–498. [Google Scholar] [CrossRef]
- Bateni, H.; Maki, B.Eastward. Assistive devices for balance and mobility: Benefits, demands, and adverse consequences. Curvation. Phys. Med. Rehabil. 2005, 86, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Chin, R.; Hsiao-Wecksler, Eastward.T.; Loth, Due east.; Kogler, Chiliad.; Manwaring, Due south.D.; Tyson, South.N.; Shorter, G.A.; Gilmer, J.N. A pneumatic power harvesting talocrural joint-foot orthosis to foreclose foot-drop. J. Neuroeng. Rehabil. 2009, half-dozen, 19. [Google Scholar] [CrossRef] [PubMed]
- Onose, Yard.; Cârdei, Five.; Crăciunoiu, Ş.T.; Avramescu, V.; Opriş, I.; Lebedev, Thousand.A.; Constantinescu, M.V. Mechatronic wearable exoskeletons for bionic bipedal standing and walking: A new synthetic approach. Front. Neurosci. 2016, 10, 343. [Google Scholar] [CrossRef]
- Lee, H.; Kim, Due west.; Han, J.; Han, C. The technical trend of the exoskeleton robot system for human power assistance. Int. J. Precis. Eng. Manuf. 2012, 13, 1491–1497. [Google Scholar] [CrossRef]
- Contreras-Vidal, J.50.; Bhagat, N.A.; Brantley, J.; Cruz-Garza, J.One thousand.; He, Y.; Manley, Q.; Nakagome, Due south.; Nathan, K.; Tan, S.H.; Zhu, F.; et al. Powered exoskeletons for bipedal locomotion afterwards spinal cord injury. J. Neural Eng. 2016, 13, 031001. [Google Scholar] [CrossRef]
- Holanda, L.J.; Silva, P.G.; Amorim, T.C.; Lacerda, M.O.; Simão, C.R.; Morya, E. Robotic assisted gait as a tool for rehabilitation of individuals with spinal cord injury: A systematic review. J. Neuroeng. Rehabil. 2017, 14, 126. [Google Scholar] [CrossRef]
- Louie, D.R.; Eng, J.J.; Lam, T. Gait speed using powered robotic exoskeletons later on spinal cord injury: A systematic review and correlational study. J. Neuroeng. Rehabil. 2015, 12, 1–10. [Google Scholar] [CrossRef]
- Esquenazi, A.; Talaty, M.; Packel, A.; Saulino, M. The ReWalk powered exoskeleton to restore ambulatory function to individuals with thoracic-level motor-complete spinal cord injury. Am. J. Phys. Med. Rehabil. 2012, 91, 911–921. [Google Scholar] [CrossRef]
- Kolakowsky-Hayner, S.A.; Coiffure, J.; Moran, S.; Shah, A. Prophylactic and feasibility of using the Ekso™ bionic exoskeleton to aid ambulation after spinal cord injury. J. Spine 2013, 4, 003. [Google Scholar]
- Quintero, H.; Farris, R.; Hartigan, C.; Clesson, I.; Goldfarb, M. A powered lower limb orthosis for providing legged mobility in paraplegic individuals. Top. Spinal Cord Inj. Rehabil. 2011, 17, 25–33. [Google Scholar] [CrossRef]
- Kilicarslan, A.; Prasad, S.; Grossman, R.One thousand.; Contreras-Vidal, J.L. High accuracy decoding of user intentions using EEG to control a lower-body exoskeleton. In Proceedings of the IEEE 2013 35th Annual International Conference of the Engineering in Medicine and Biology Society (EMBC), Osaka, Nippon, 3–7 July 2013; pp. 5606–5609. [Google Scholar]
- He, Y.; Eguren, D.; Azorín, J.Thou.; Grossman, R.Thousand.; Luu, T.P.; Contreras-Vidal, J.50. Encephalon—Car interfaces for controlling lower-limb powered robotic systems. J. Neural Eng. 2018, xv, 021004. [Google Scholar] [CrossRef]
- Simic, K.; Tariq, 1000.; Trivailo, P. EEG-Based BCI Control Schemes for Lower-Limb Assistive-Robots. Front. Hum. Neurosci. 2018, 12, 312. [Google Scholar]
- Suzuki, K.; Mito, K.; Kawamoto, H.; Hasegawa, Y.; Sankai, Y. Intention-based walking support for paraplegia patients with Robot Suit HAL. Adv. Robot. 2007, 21, 1441–1469. [Google Scholar] [CrossRef]
- Veneman, J.F. Exoskeletons supporting postural balance—The Residual project. In Supervene upon, Repair, Restore, Salvage—Bridging Clinical and Engineering Solutions in Neurorehabilitation; Springer: Cham, Switzerland, 2014; pp. 203–208. [Google Scholar]
- Choi, H.; Na, B.; Kim, S.; Lee, J.; Kim, H.; Kim, D.; Cho, D.; Kim, J.; Shin, S.; Rha, D.West.; et al. Affections-arrange: A modularized lower-limb wearable robot for assistance of people with partially impaired walking ability. In Proceedings of the IEEE 2019 Clothing Robotics Association Conference (WearRAcon), Scottsdale, AZ, USA, 26–28 March 2019; pp. 51–56. [Google Scholar]
- ReWalk ReStore. Bachelor online: https://rewalk.com/restore/ (accessed on 27 March 2021).
- Oh, S.; Kong, K. High-precision robust strength command of a series elastic actuator. IEEE/ASME Trans. Mechatron. 2017, 22, 71–80. [Google Scholar] [CrossRef]
- Lee, C.; Kwak, S.; Kwak, J.; Oh, S. Generalization of Series Elastic Actuator configurations and dynamic behavior comparison. Actuators 2017, 6, 26. [Google Scholar] [CrossRef]
- Dos Santos, W.Yard.; Caurin, G.A.; Siqueira, A.A. Pattern and command of an active knee orthosis driven past a rotary series elastic actuator. Control Eng. Pract. 2017, 58, 307–318. [Google Scholar] [CrossRef]
- Srivastava, S.; Kao, P.C.; Reisman, D.S.; Scholz, J.P.; Agrawal, S.K.; Higginson, J.South. Robotic assist-every bit-needed as an alternative to therapist-assisted gait rehabilitation. Int. J. Phys. Med. Rehabil. 2016, iv, 370. [Google Scholar] [CrossRef]
- Simonsen, East.B.; Cappelen, Chiliad.L.; Skorini, R.I.; Larsen, P.K.; Alkjær, T.; Dyhre-Poulsen, P. Explanations pertaining to the hip joint flexor moment during the stance stage of homo walking. J. Appl. Biomech. 2012, 28, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Alkjær, T.; Larsen, P.K.; Pedersen, G.; Nielsen, 50.H.; Simonsen, E.B. Biomechanical analysis of rollator walking. Biomed. Eng. Online 2006, 5, ii. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.; Herzog, Westward.; Nigg, B. Use of forcefulness platform variables to quantify the furnishings of chiropractic manipulation on gait symmetry. J. Manip. Physiol. Ther. 1987, 10, 172–176. [Google Scholar]
- Waters, R.50.; Mulroy, S. The energy expenditure of normal and pathologic gait. Gait Posture 1999, 9, 207–231. [Google Scholar] [CrossRef]
Effigy 1. Angel Legs, a lower-extremity powered exoskeleton for assisting joint torques [19].
Figure 1. Angel Legs, a lower-extremity powered exoskeleton for assisting articulation torques [xix].

Figure ii. AngelJoint v1: (a) the outside view and (b) the structure of the series elastic actuation system.
Figure ii. AngelJoint v1: (a) the outside view and (b) the structure of the series elastic actuation system.
Effigy three. Linearity of bound embedded in gears.
Figure 3. Linearity of bound embedded in gears.
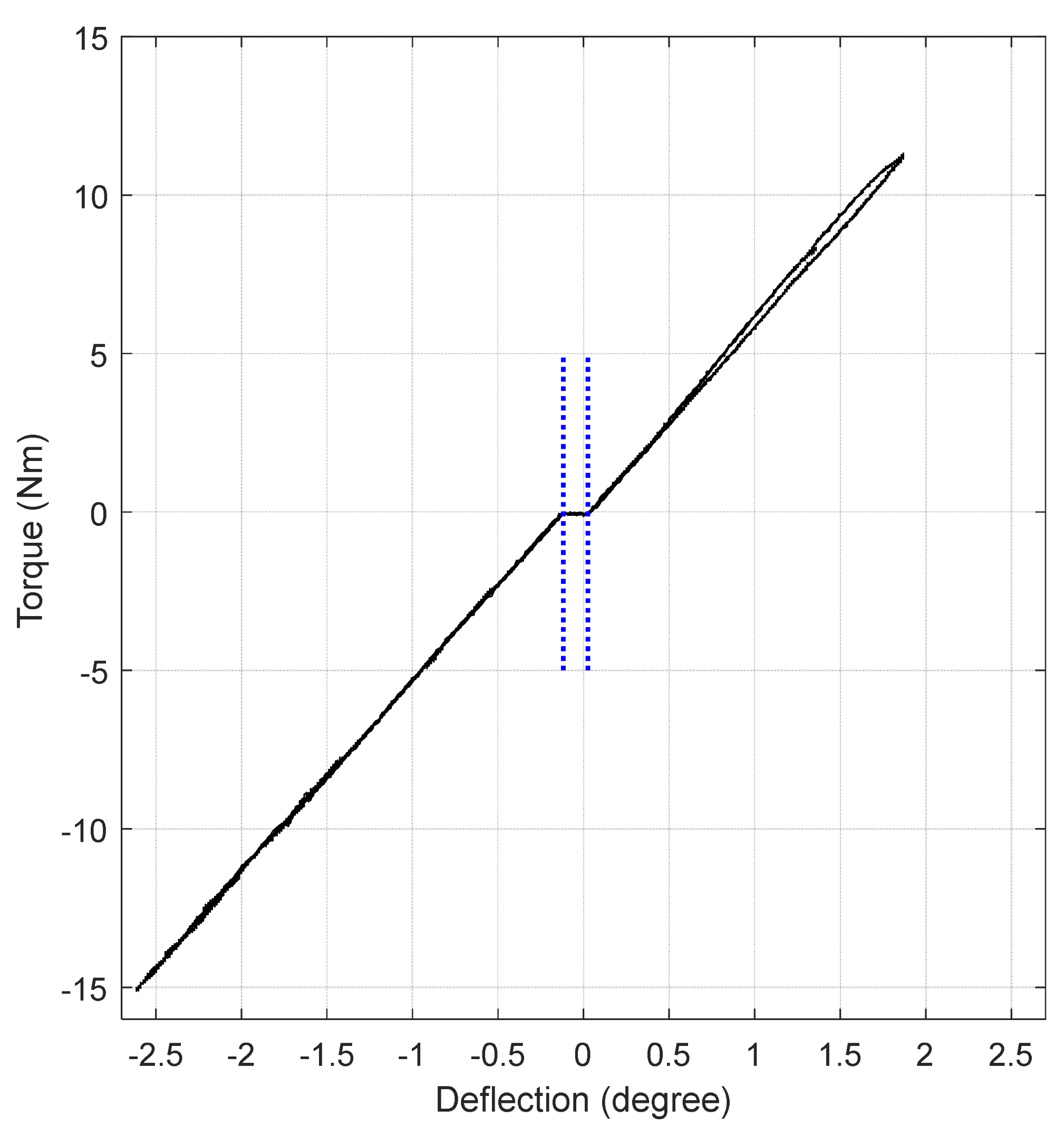
Figure 4. Assistive torque command of the series elastic actuation (SEA) module.
Figure 4. Assistive torque control of the series elastic actuation (Ocean) module.
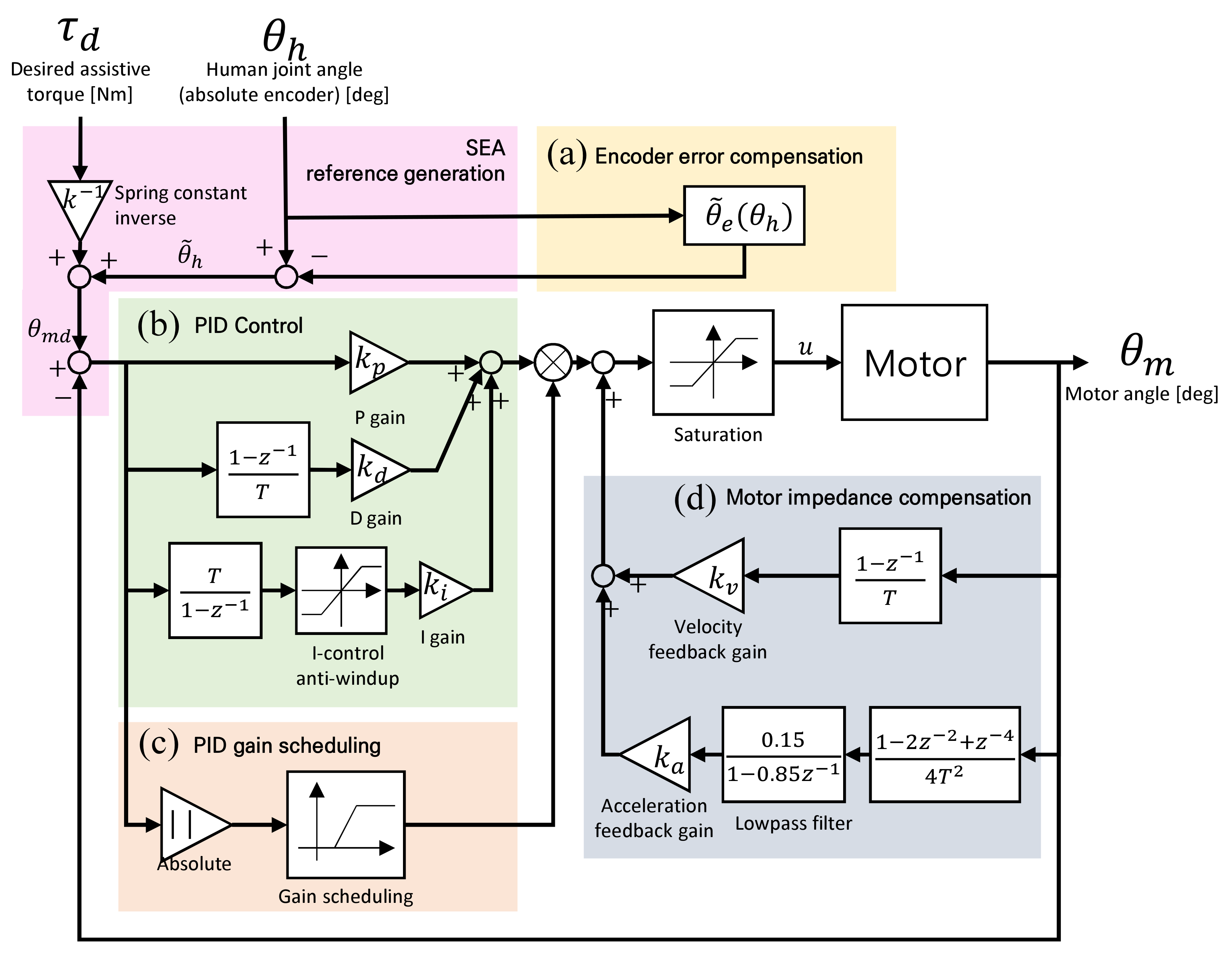
Figure v. Gait patterns of a leg: 1 gait cycle is from when the foot initially contacts the basis to when the foot contacts the footing again. DS1 and DS2 mean the first and the second double limb back up phases, respectively.
Figure 5. Gait patterns of a leg: i gait cycle is from when the pes initially contacts the ground to when the human foot contacts the ground again. DS1 and DS2 hateful the first and the 2d double limb support phases, respectively.
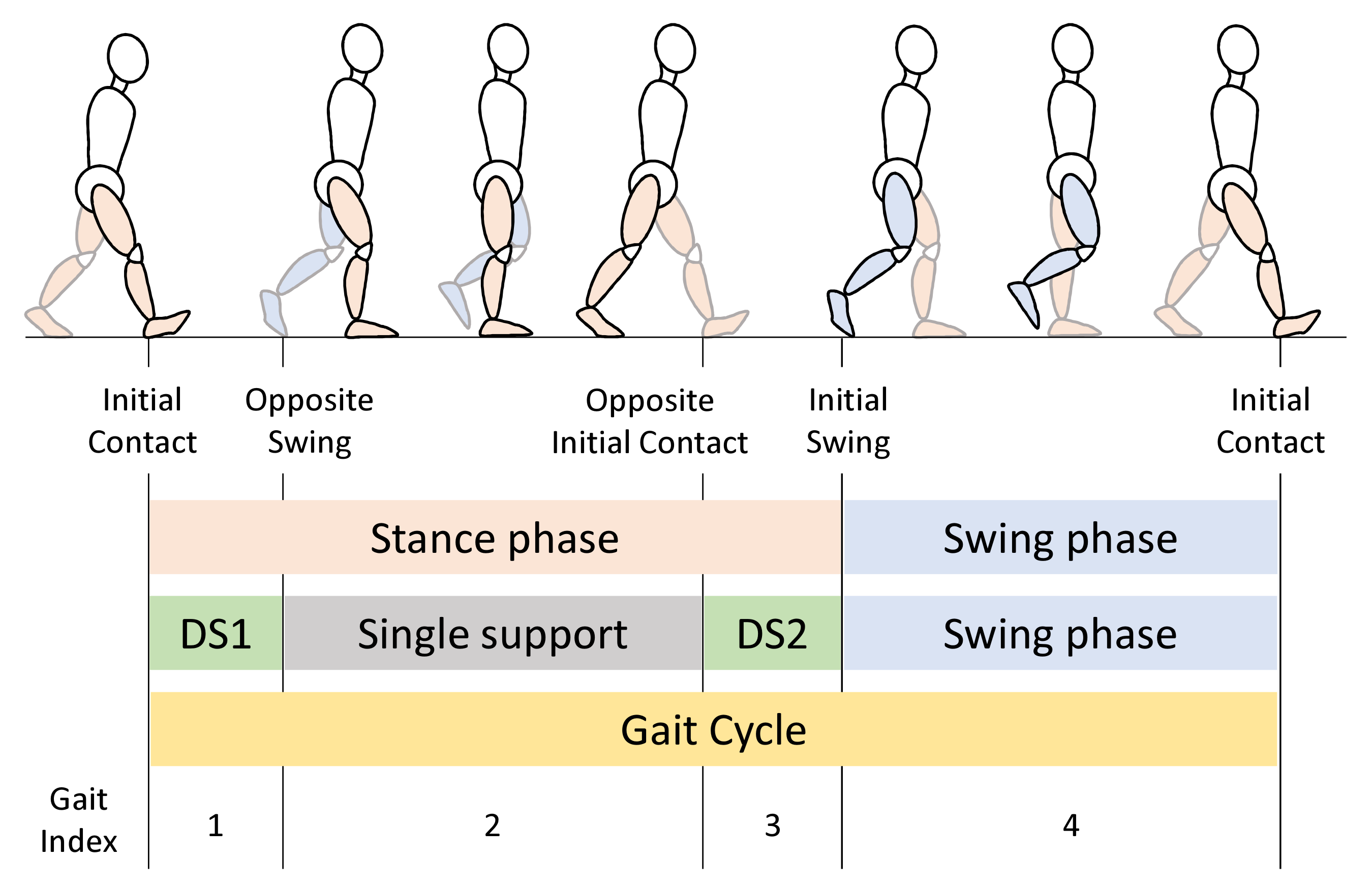
Figure vi. Gait index measurement results: (a) swing phases of both legs. Values of 1 stand for the swing phase and values of 0 stand for the stance phases. (b) Representative gait index.Gait alphabetize measurement results.
Effigy vi. Gait index measurement results: (a) swing phases of both legs. Values of i represent the swing stage and values of 0 represent the stance phases. (b) Representative gait alphabetize.Gait index measurement results.
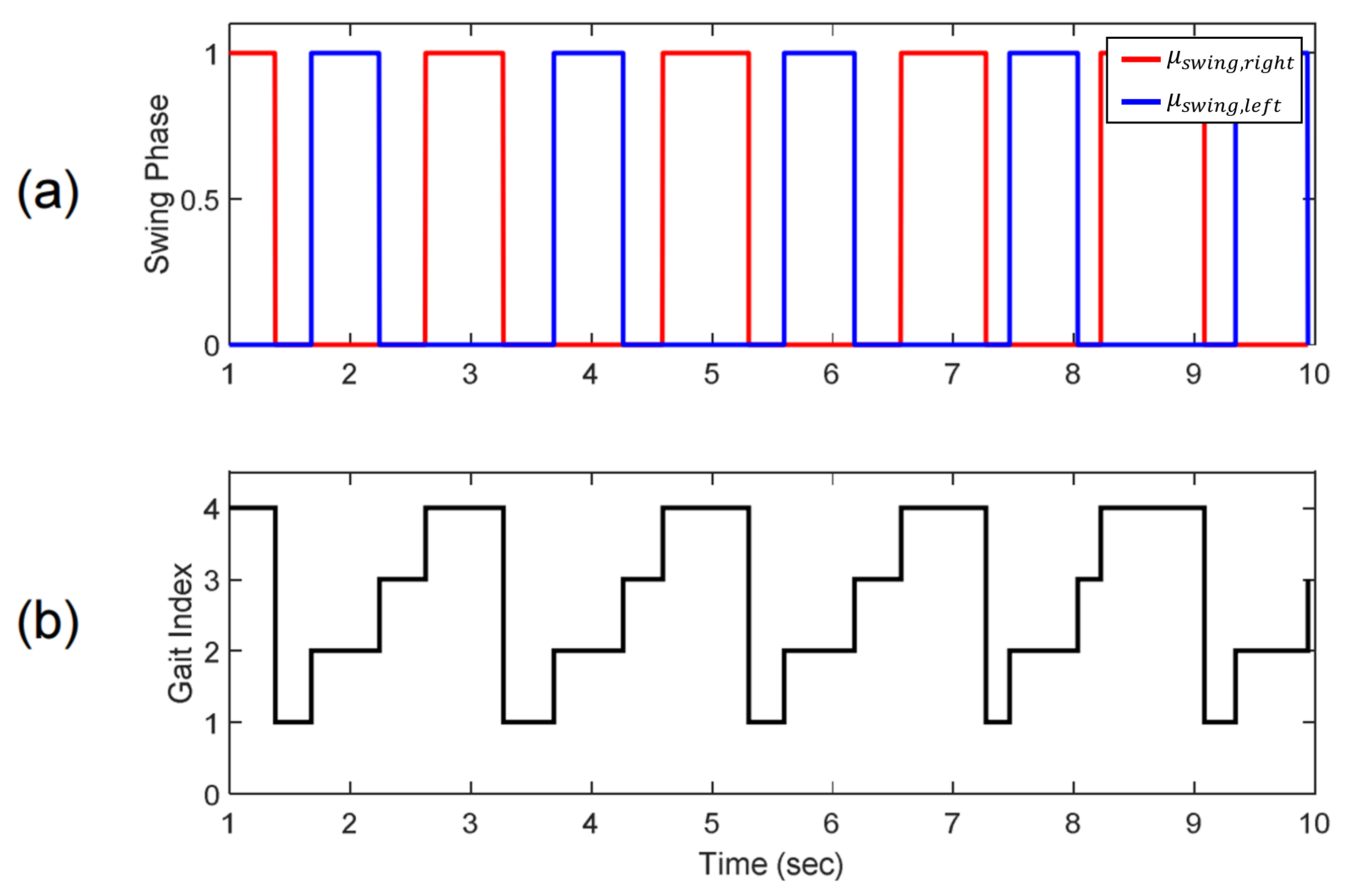
Figure 7. The overall control structure of Angel Legs.
Figure 7. The overall control structure of Angel Legs.
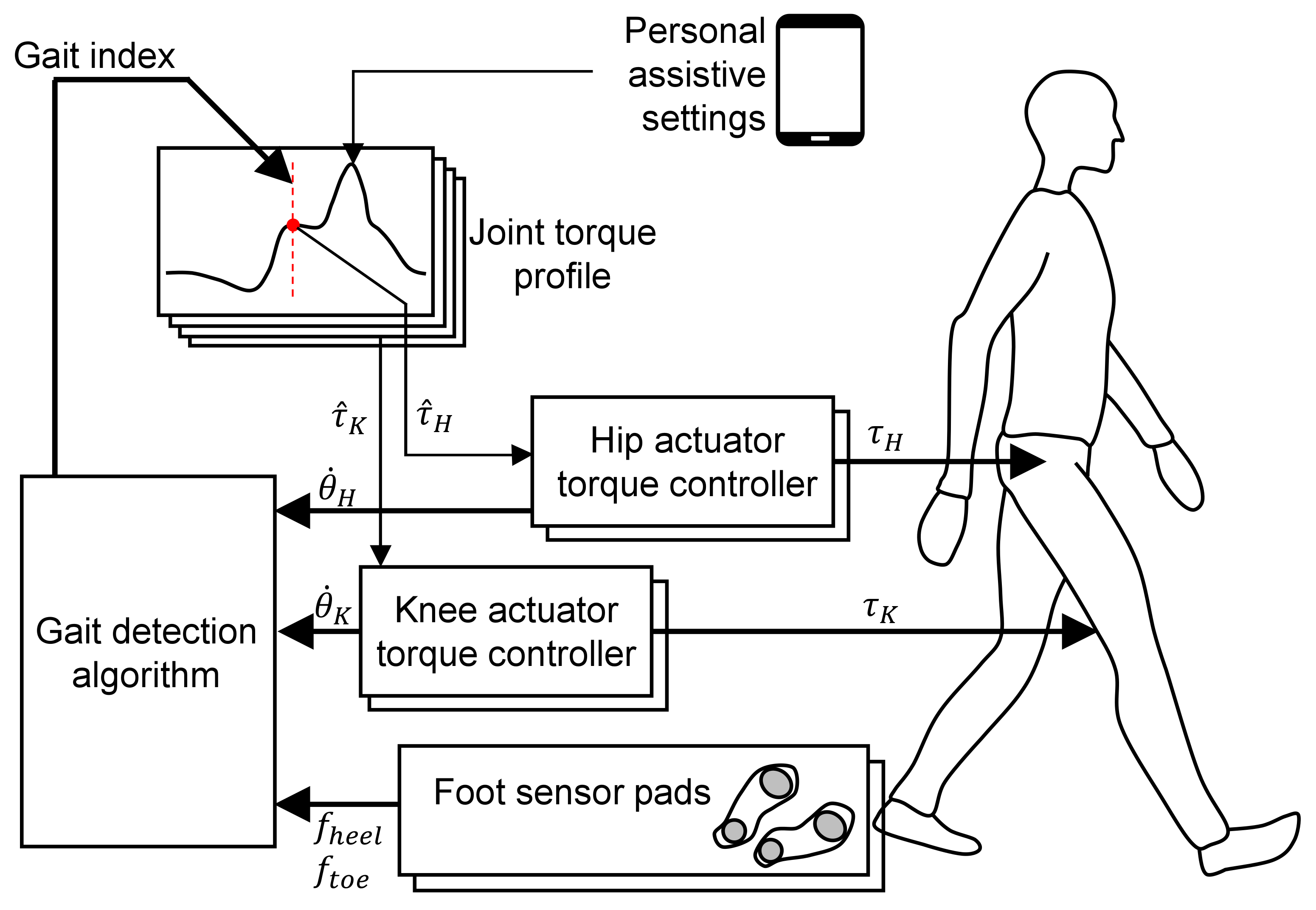
Figure eight. Assistive torque profile functions of hip and knee joints during a gait bicycle: (a) the initial contact issue of a leg, (b) the reverse foot-off outcome, (c) the initial contact of the opposite leg, (d) the pes-off (i.due east., initial swing) issue, and (e) the end of the gait (i.due east., initial contact event of the next step).
Figure 8. Assistive torque profile functions of hip and articulatio genus joints during a gait bike: (a) the initial contact event of a leg, (b) the contrary foot-off event, (c) the initial contact of the opposite leg, (d) the foot-off (i.eastward., initial swing) consequence, and (east) the end of the gait (i.e., initial contact event of the next stride).
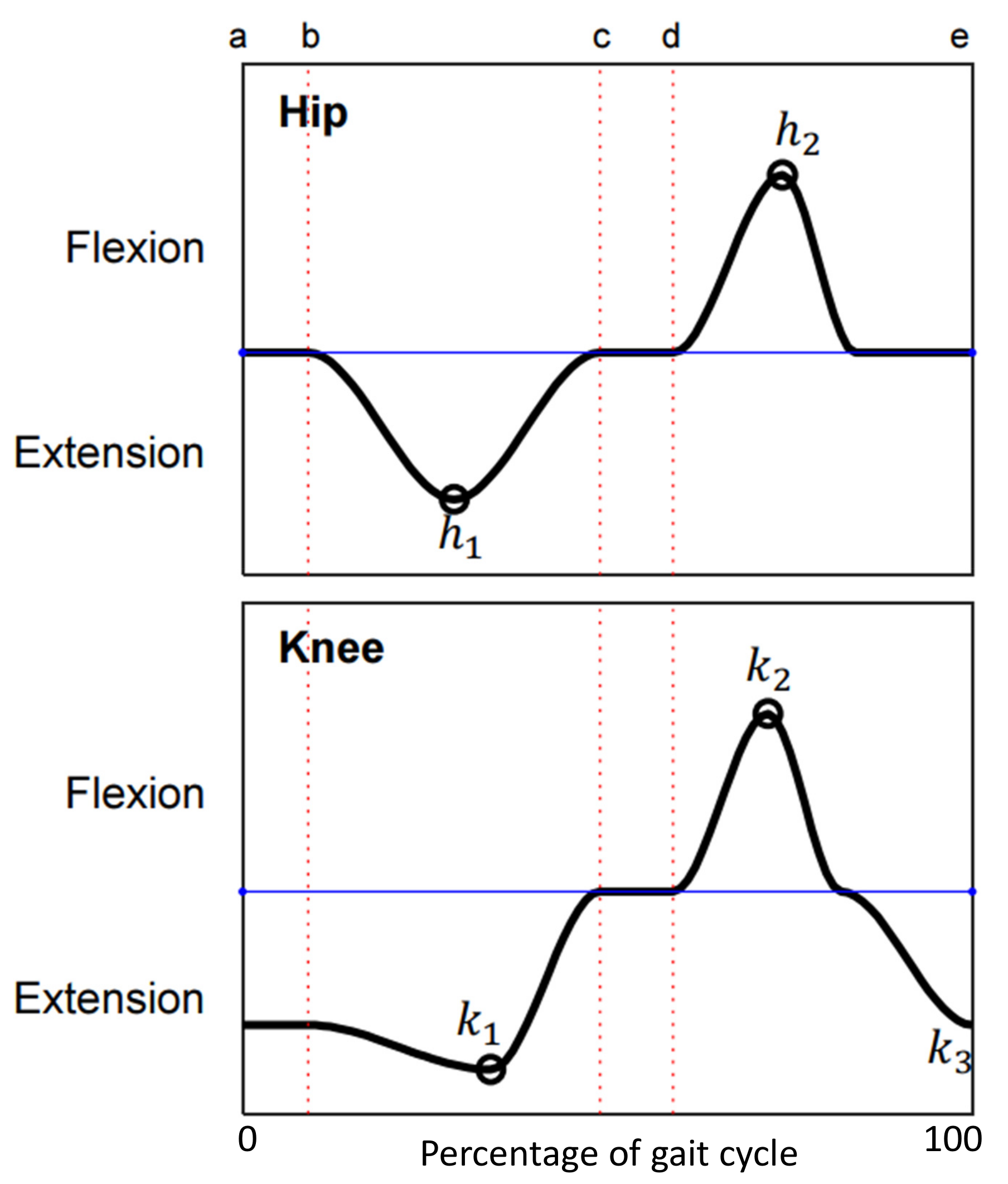
Figure nine. Gait analysis of a patient with spina bifida wearing Talocrural joint Foot Orthosis (AFO) and using a walker.
Figure 9. Gait analysis of a patient with spina bifida wearing Ankle Foot Orthosis (AFO) and using a walker.
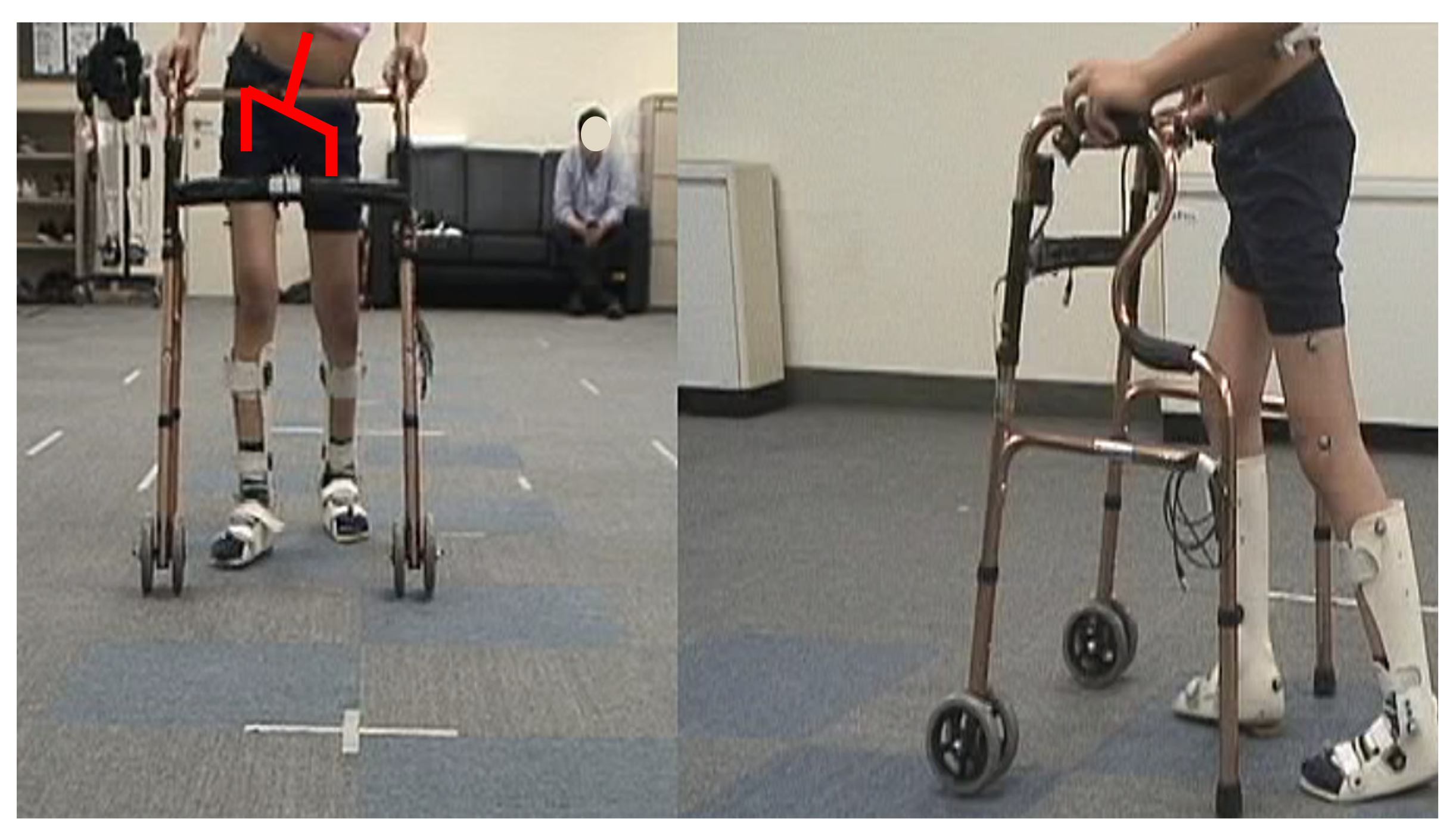
Figure 10. Robotic gait grooming protocol.
Effigy 10. Robotic gait training protocol.
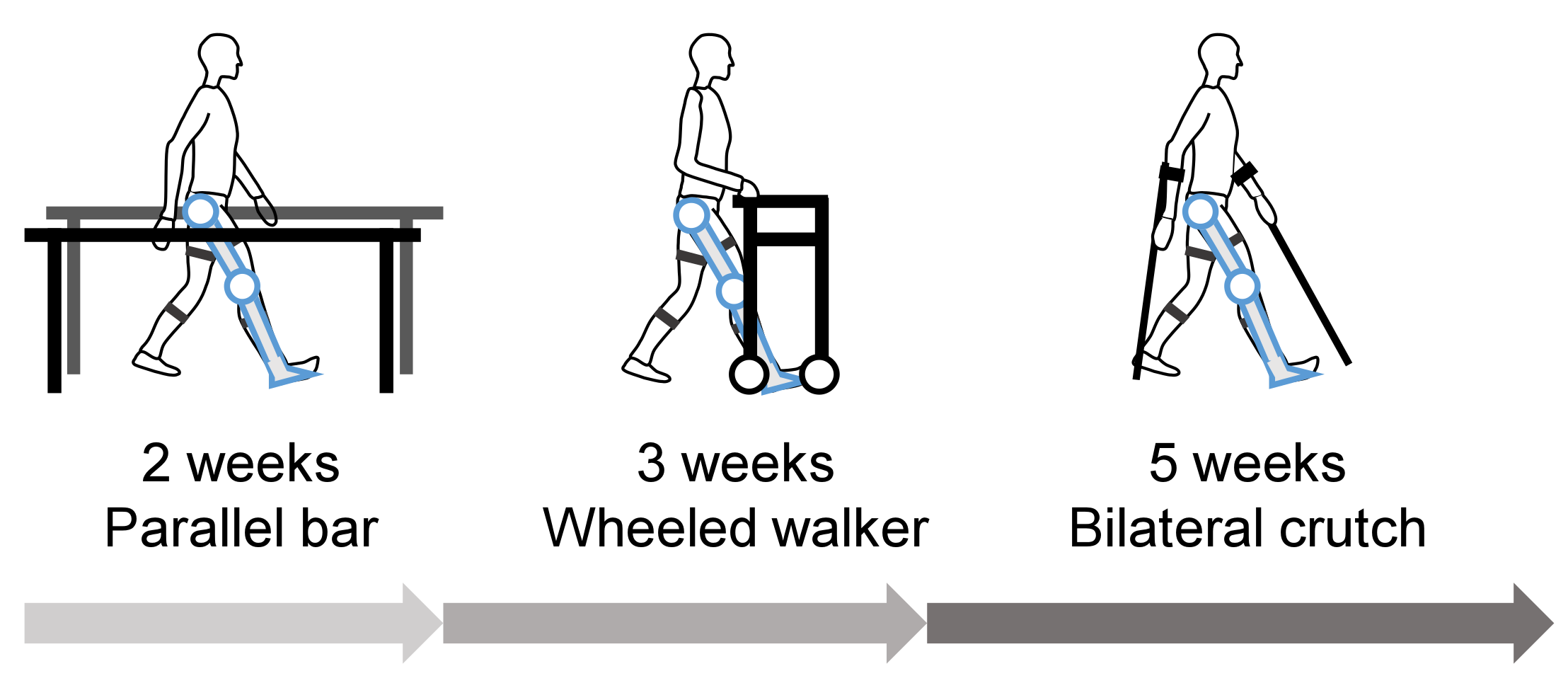
Figure 11. Kinematic issue of a patient with spina bifida with Affections Legs and using parallel confined. The solid gray line represents data without Angel Legs, the light blue line represents data with Angel Legs without assistive command, and the red line represents data with assistive control. Vertical lines represents the gait phases. Dotted vertical lines represent the unmarried limb support phase (opposite human foot off), dashed vertical lines correspond the second double limb support phase (opposite foot contact), and solid vertical lines represent initial swing.
Figure eleven. Kinematic issue of a patient with spina bifida with Affections Legs and using parallel confined. The solid greyness line represents data without Angel Legs, the light blue line represents data with Angel Legs without assistive control, and the scarlet line represents data with assistive control. Vertical lines represents the gait phases. Dotted vertical lines correspond the single limb back up phase (opposite pes off), dashed vertical lines represent the second double limb support phase (opposite foot contact), and solid vertical lines represent initial swing.
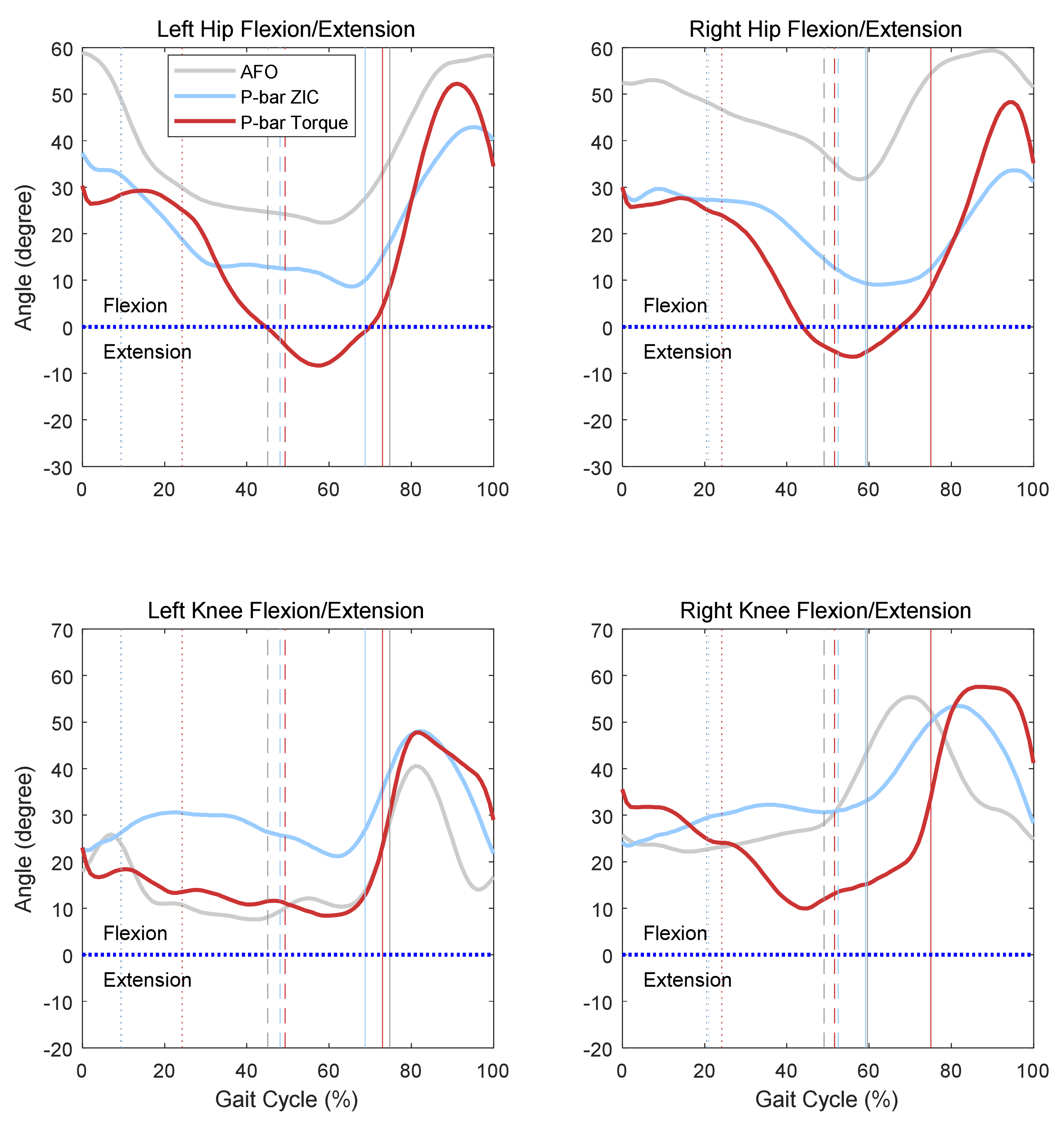
Figure 12. Gait training of a patient with spina bifida with Affections Legs and using a wheeled walker.
Figure 12. Gait grooming of a patient with spina bifida with Angel Legs and using a wheeled walker.

Figure 13. Kinematic result of a walking trial wearing a torque-controlled robotic device and using a wheeled walker. The start vertical dashed lines represent the unmarried limb support stage (opposite human foot off), the second vertical dashed lines represent the second double limb support phase (opposite foot contact), and the solid vertical lines represent initial swing.
Effigy xiii. Kinematic outcome of a walking trial wearing a torque-controlled robotic device and using a wheeled walker. The showtime vertical dashed lines correspond the single limb support stage (opposite foot off), the second vertical dashed lines represent the second double limb support phase (reverse human foot contact), and the solid vertical lines represent initial swing.
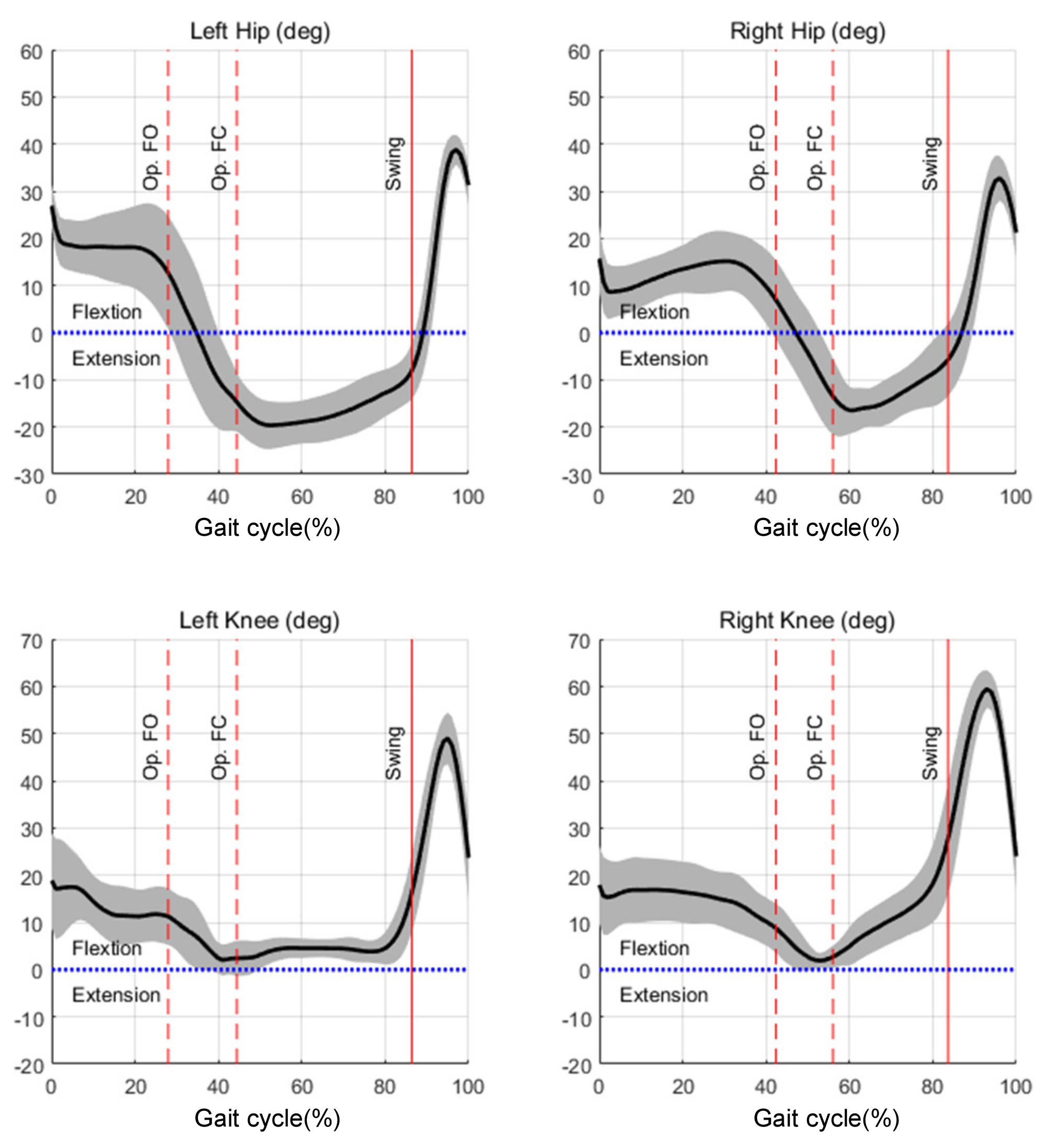
Figure 14. Walking trial of a patient with spina bifida wearing Angel Legs and using bilateral forearm crutches.
Effigy 14. Walking trial of a patient with spina bifida wearing Angel Legs and using bilateral forearm crutches.

Effigy 15. Kinematic results of five-calendar week walking training with Affections Legs and using bilateral crutches. The bright lines represent the early stages of training, and the dark lines represent the afterwards stages of the training. Vertical lines stand for the start of swing phase.
Figure 15. Kinematic results of v-week walking training with Affections Legs and using bilateral crutches. The bright lines represent the early stages of training, and the night lines represent the after stages of the training. Vertical lines stand for the starting time of swing phase.
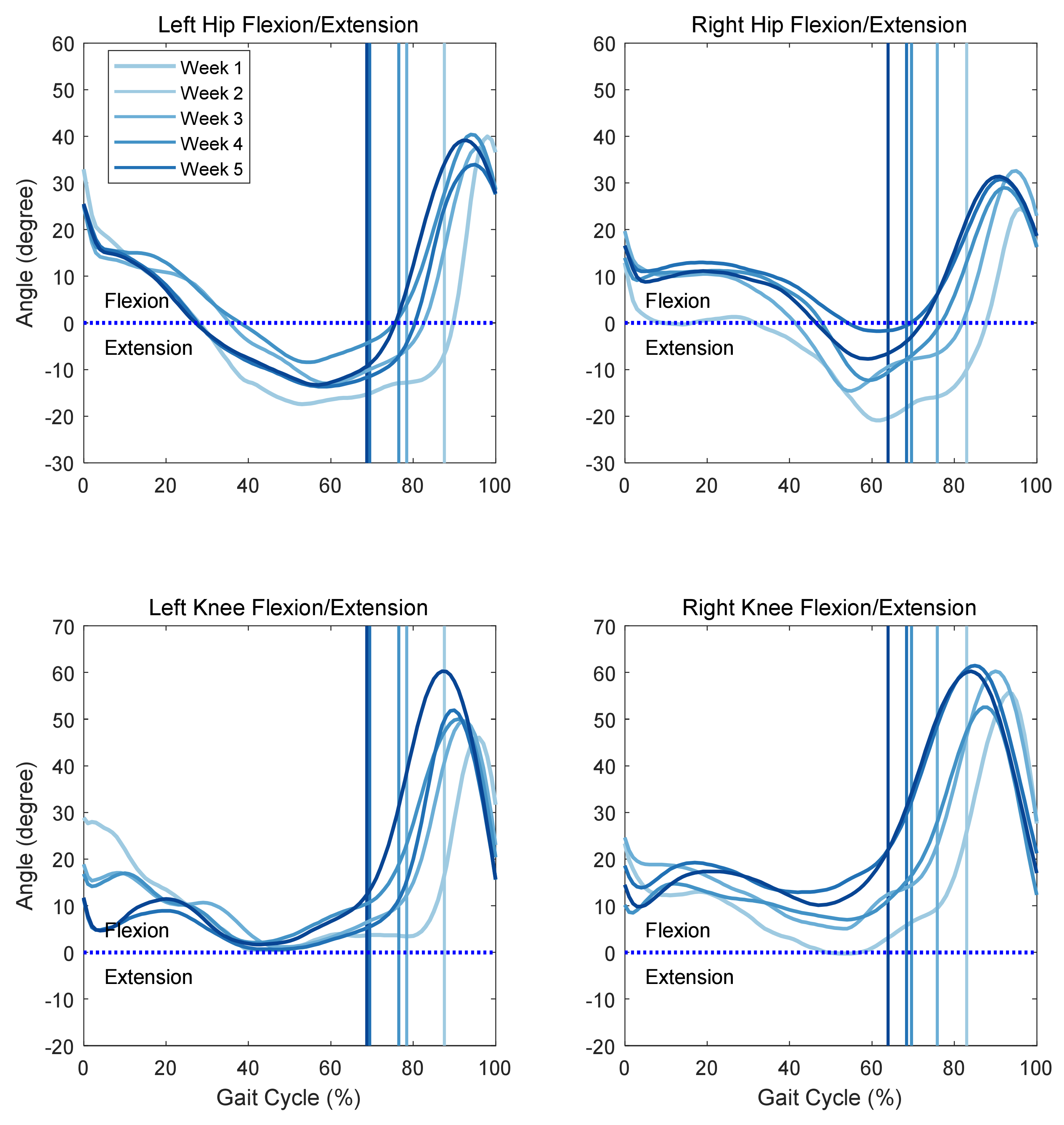
Figure 16. Results of five-calendar week walking preparation with Angel Legs and using bilateral crutches. (a) Percentage of stance phase and single limb support (opposite foot-off) time of left and right legs. (b) Percentage of double limb support time during a gait. (c) Percent of unmarried limb support time during a gait.
Figure 16. Results of v-week walking preparation with Affections Legs and using bilateral crutches. (a) Percentage of opinion phase and single limb support (opposite foot-off) time of left and right legs. (b) Pct of double limb back up fourth dimension during a gait. (c) Pct of single limb support time during a gait.
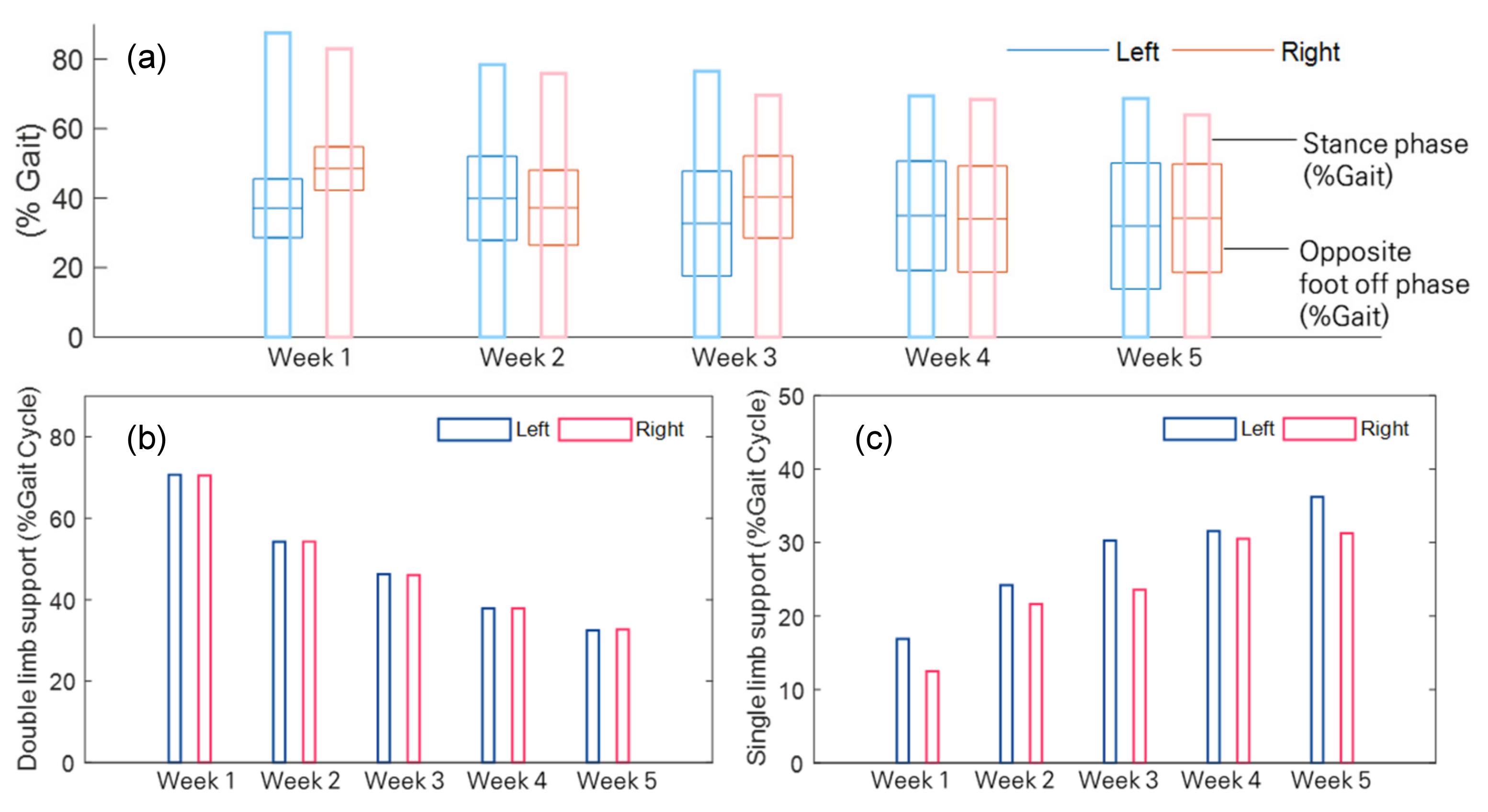
Figure 17. Kinematic results of gait analysis of walking using bilateral crutches. The solid pinkish line represents information without robotic assist, and the solid black line represents information with assistance. The showtime vertical dashed lines represent the single limb back up phase (opposite pes-off), 2d vertical dashed lines represent the second double limb support phase (opposite foot contact), and the solid vertical lines represent the swing phase.
Figure 17. Kinematic results of gait analysis of walking using bilateral crutches. The solid pink line represents data without robotic assistance, and the solid black line represents information with aid. The first vertical dashed lines stand for the unmarried limb back up stage (opposite foot-off), second vertical dashed lines represent the 2d double limb back up phase (contrary foot contact), and the solid vertical lines represent the swing phase.
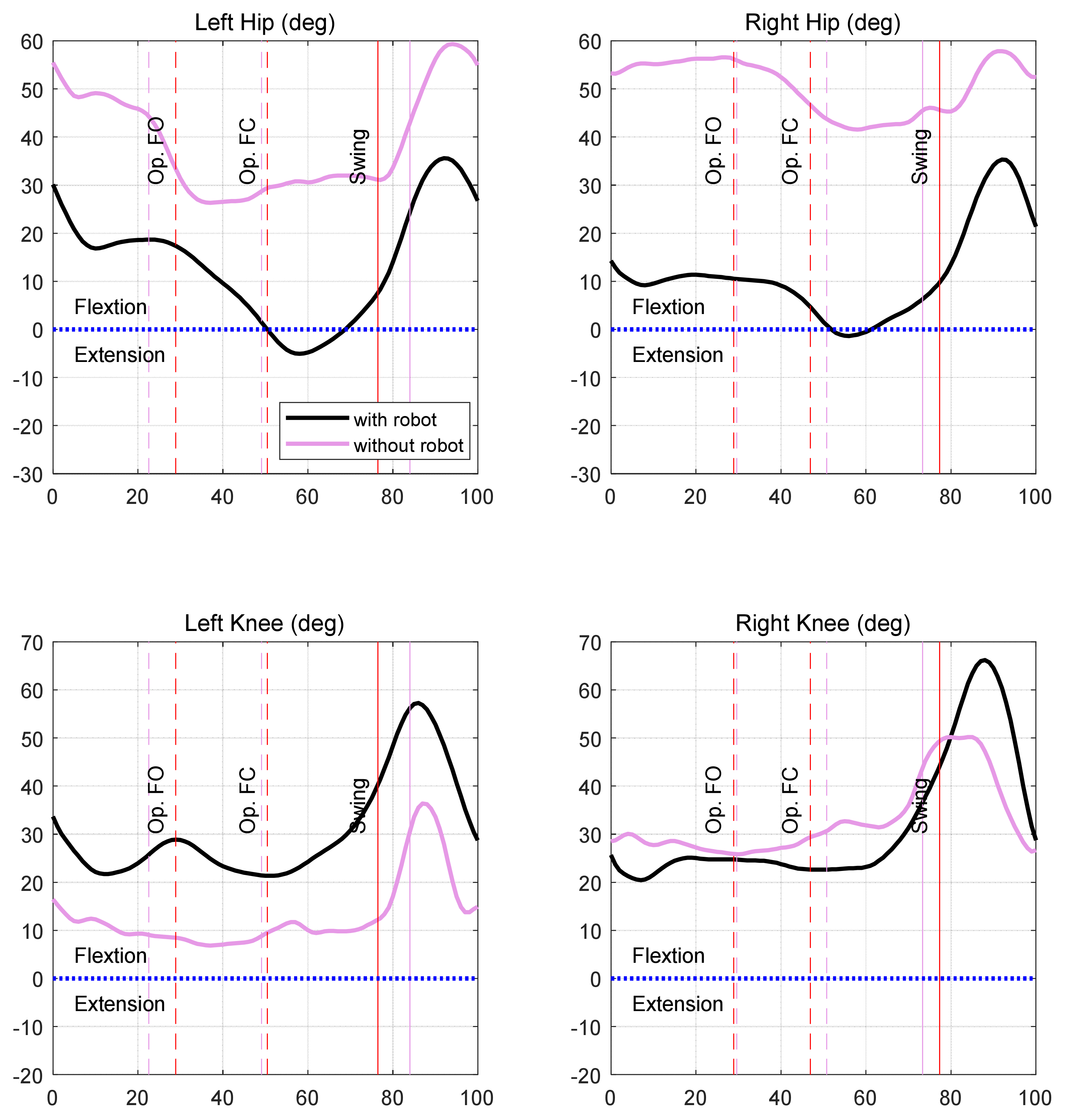
Figure 18. Applied torque profiles of iii trials for (a) left hip joint, (b) right hip joint, (c) left articulatio genus articulation, and (d) right knee joint. Only the extension torques of the correct knee joint were different in each case.Applied torque profiles of three trials.
Figure 18. Applied torque profiles of 3 trials for (a) left hip joint, (b) right hip joint, (c) left articulatio genus articulation, and (d) right knee articulation. Only the extension torques of the right knee joint were different in each case.Applied torque profiles of iii trials.
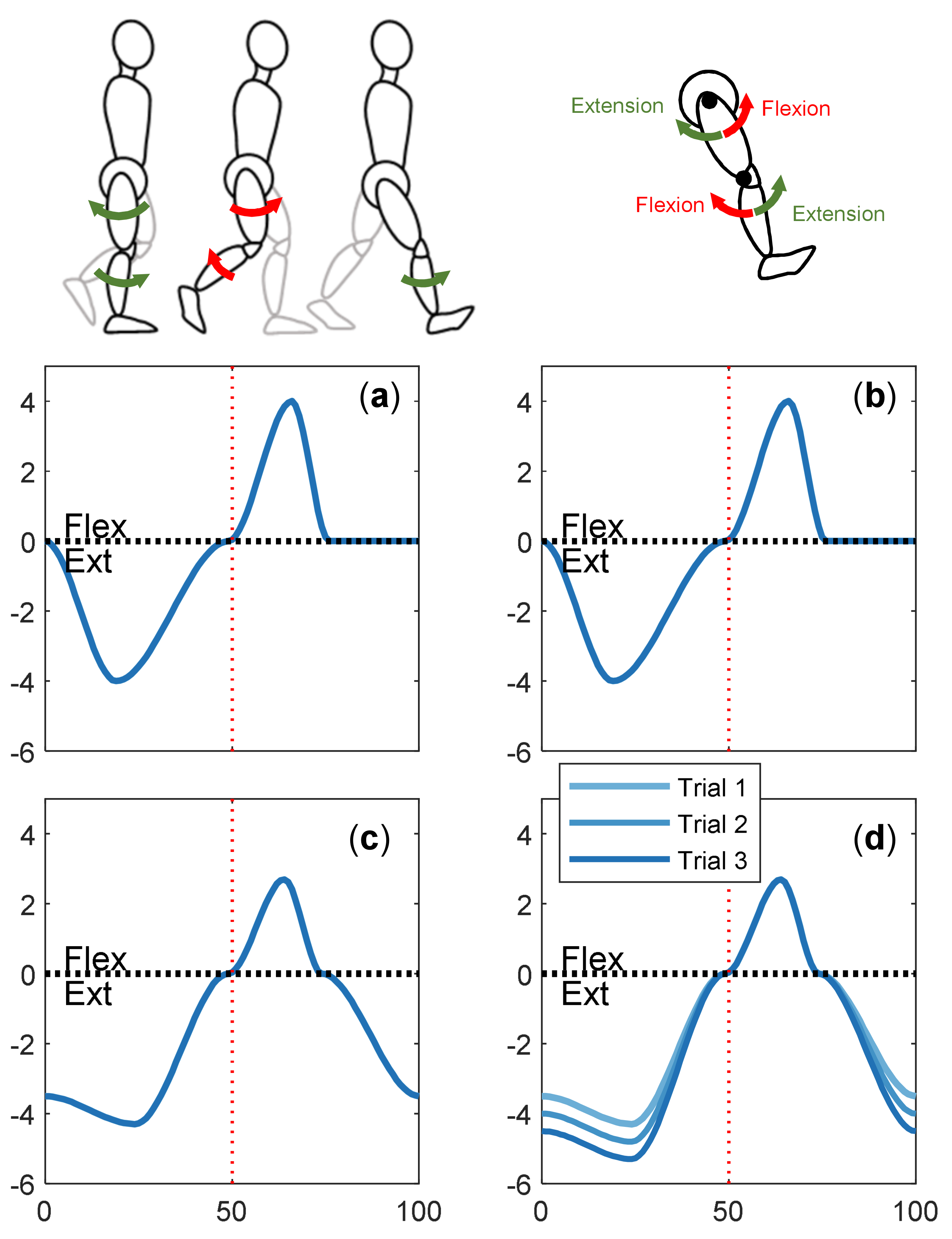
Figure 19. Kinematic results of walking trials with the three dissimilar right knee assistive levels.
Figure 19. Kinematic results of walking trials with the three dissimilar correct knee joint assistive levels.
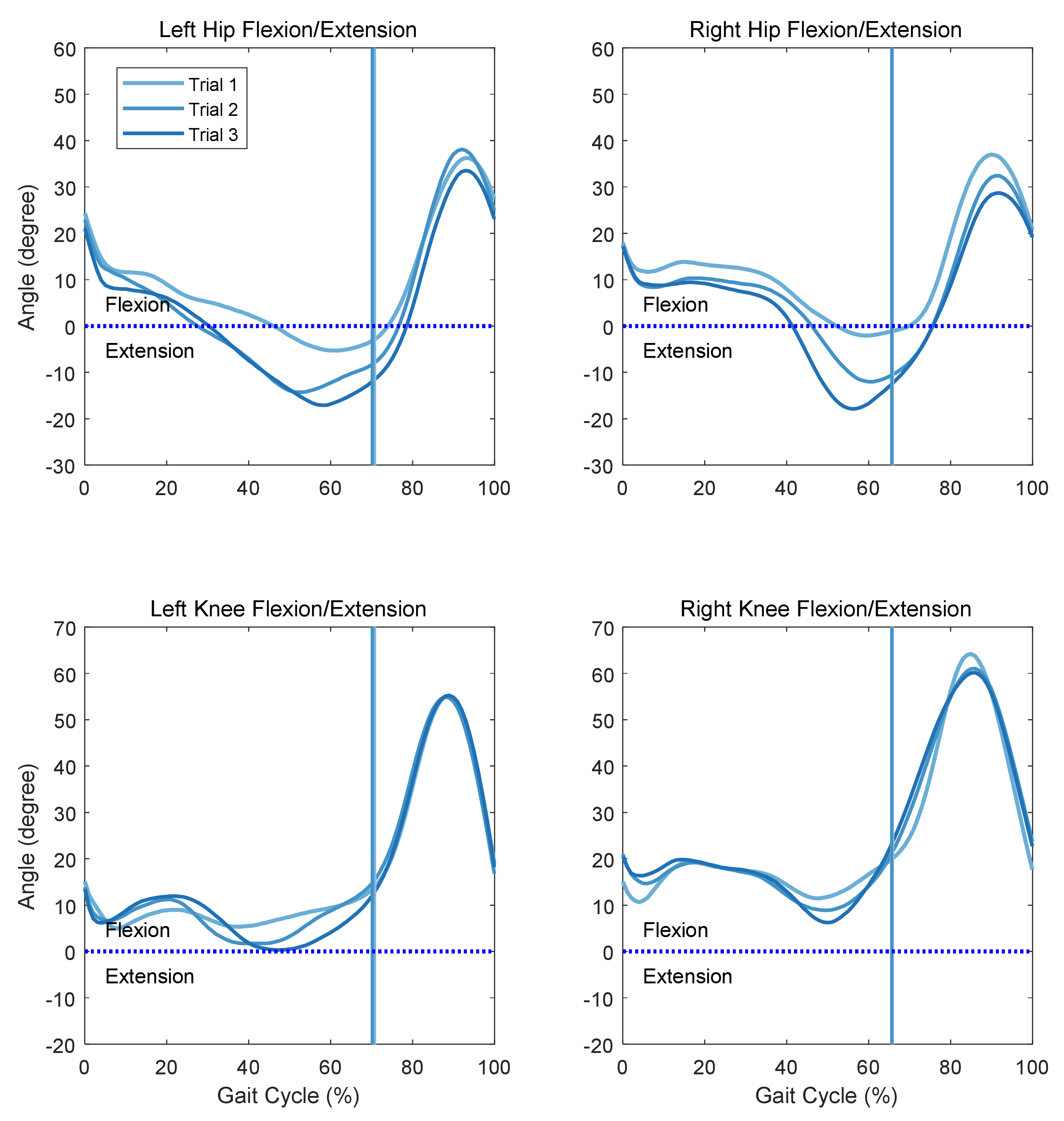
Table 1. Specification of Affections Joint v1.
Table i. Specification of Affections Joint v1.
| Spec | Unit | Value |
|---|---|---|
| Dimension | W × D × H [mm] | |
| Weight | [kg] | 0.76 |
| Assistive torque | [Nm] | xiv.two (cont.), 35.5 (peak) |
| Maximum speed | [rpm] | 66.4 |
| Range of motion | [deg] | 170 |
Table ii. Gait parameters of walker gait wearing a torque-controlled robot.
Table two. Gait parameters of walker gait wearing a torque-controlled robot.
| Left | Correct | |
|---|---|---|
| Gait period (s) | 4.11 | 4.08 |
| Stance period (southward) | iii.56 | 3.43 |
| Opinion catamenia (%GC) | 86.39 | 86.63 |
| Opposite human foot contact (%GC) | 44.40 | 56.03 |
| Contrary foot off (%GC) | 27.95 | 42.33 |
| Range of hip movement (degree) | 58.44 (–19.62 38.82) | 49.21 (–sixteen.47 32.73) |
| Range of genu motion (degree) | 46.91 (2.06 48.97) | 57.53 (1.89 59.42) |
Tabular array iii. Oxygen costs of the half dozen-min metabolic test of walking without and with Angel Legs using a wheeled walker.
Table 3. Oxygen costs of the half dozen-min metabolic exam of walking without and with Angel Legs using a wheeled walker.
| Without Assistance | Robot Aid | |
|---|---|---|
| Oxygen price (mL/kg/m) |
Table four. Gait parameters of bilateral crutches gait with Angel Legs.
Table 4. Gait parameters of bilateral crutches gait with Affections Legs.
| Left | Right | |
|---|---|---|
| Gait period (s) | 2.04 | 1.94 |
| Stance period (due south) | i.56 | 1.fifty |
| Opinion menstruation (%GC) | 76.47 | 77.32 |
| Contrary foot contact (%GC) | 50.49 | 46.91 |
| Opposite foot off (%GC) | 28.92 | 28.87 |
| Range of hip motion (degree) | 40.68 (–5.08 35.59) | 36.68 (–1.36 35.32) |
| Range of knee motility (caste) | 35.91 (21.34 57.24) | 45.77 (20.42 66.19) |
Table five. Oxygen costs of the 6-min metabolic test of walking without help and walking with Angel Legs using bilateral crutches.
Tabular array 5. Oxygen costs of the half-dozen-min metabolic exam of walking without help and walking with Affections Legs using bilateral crutches.
| Without Assistance | Robot Assistance | |
|---|---|---|
| Oxygen cost (mL/kg/m) |
Table 6. Gait analysis results of trials.
Table six. Gait analysis results of trials.
| Without Robot Assistance | Robot Aid Trial i | Robot Assist Trial 2 | Robot Assist Trial 3 | ||
|---|---|---|---|---|---|
| Gait bicycle (southward) | L | 2.75 | 2.28 | 2.ten | 1.93 |
| R | 2.74 | 2.27 | 2.11 | one.93 | |
| Get-go double support | L | 22.55 | 12.49 | 12.64 | xvi.88 |
| (%Gait) | R | 29.56 | 24.13 | 23.46 | xviii.58 |
| Single support | L | 26.55 | 34.eighteen | 34.45 | 34.thirty |
| (%Gait) | R | 21.17 | 29.31 | 29.24 | xxx.xvi |
| Second double back up | 50 | 34.91 | 24.thirteen | 23.49 | 18.96 |
| (%Gait) | R | 22.63 | 12.41 | 12.91 | 16.93 |
| Stance phase | Fifty | 84.00 | 70.80 | lxx.58 | seventy.fifteen |
| (%Gait) | R | 73.36 | 65.87 | 65.61 | 65.68 |
| Maximum hip extension | 50 | 26.32 | –5.32 | –14.32 | –17.12 |
| (deg) | R | 41.58 | –2.08 | –12.06 | –17.91 |
| Publisher's Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the writer. Licensee MDPI, Basel, Switzerland. This commodity is an open admission article distributed under the terms and conditions of the Creative Commons Attribution (CC Past) license (https://creativecommons.org/licenses/by/4.0/).
Source: https://www.mdpi.com/2076-3417/11/7/3114/htm